Autism is not a niche issue. It is a system design failure India can no longer ignore.
Families don't struggle because care doesn't exist. They struggle because nothing connects. Diagnosis here. Therapy there. School support somewhere else. No one is in charge of the whole picture.

Why the system fails
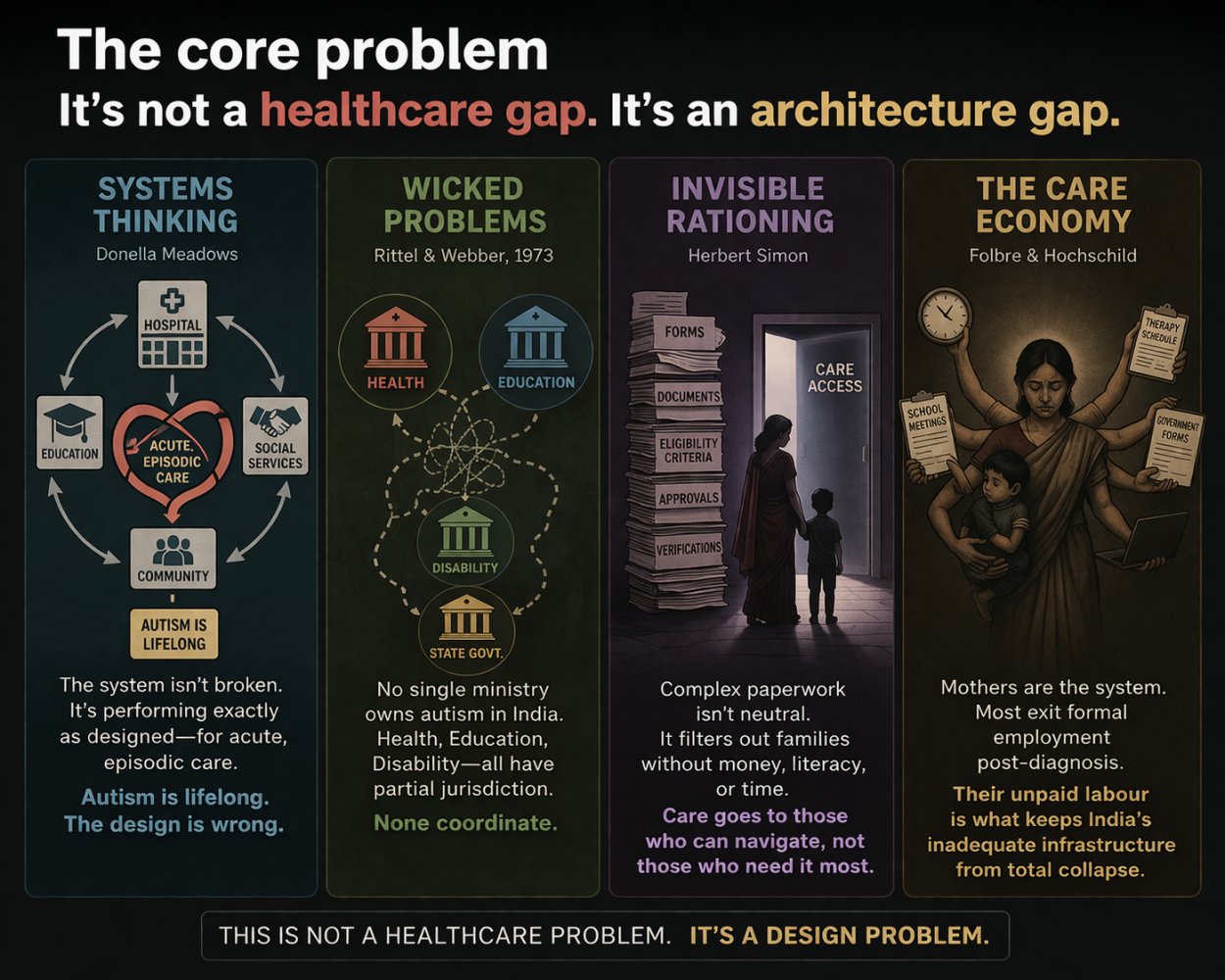
Five frameworks explain why India's autism ecosystem produces the outcomes it does.
The system produces exactly what it is designed to produce
India's autism ecosystem isn't broken. It's designed for acute, episodic care, not lifelong neurodevelopmental support. Fragmentation, poor transitions and disconnected data aren't failures. They're outcomes of the wrong system goal.
Complex systems do not treat everyone equally
Administrative complexity quietly filters access. Families with resources navigate it; others are excluded. Care is often allocated not by need, but by the ability to manage bureaucracy.
No single owner means no integrated solution
Autism spans health, education, disability and employment. Every stakeholder owns a piece; no one owns the whole. The result is systemic fragmentation by design.
The problem is not the individual. It is the environment.
India's system still focuses on "fixing" individuals. The shift required is toward designing inclusive schools, workplaces and communities that accommodate difference.
The system runs on invisible labour
Mothers are the backbone of autism care in India. Their unpaid, unrecognized labour keeps the system functioning despite structural gaps.
You cannot redesign a system you cannot see. India cannot see most of its autism ecosystem, because it has chosen not to measure it.
Why India's autism crisis runs deeper than a service shortage
Applying the 5 Whys reveals the problem isn't merely insufficient services. It's a systemic design failure layered at every level.
Why are families struggling to get support?
Medical, educational and social services rarely communicate. Diagnosis takes months or years. Stigma drives social withdrawal. Professionals themselves often lack awareness, compounding the burden.
Why are services so fragmented?
India needs over 2 million special educators but has only 12,000–15,000. A 2021 Supreme Court directive requiring one per school left 150,000 positions unfilled. With 0.75 psychiatrists per 100,000 people, families pay privately, often forcing mothers out of the workforce.
Why is there such a workforce gap?
Training pipelines are underdeveloped because autism has historically been treated as niche. Medical schools have neglected specialized curricula. Pathways for adolescents and adults are almost nonexistent.
Why has autism remained a low policy priority?
Cultural stigma suppresses demand and enables governments to deprioritise investment. Families report providers and educators associating neurodevelopmental differences with "bad parenting", keeping autism politically invisible.
Why is awareness and data still so limited?
India lacks comprehensive disability data. Without reliable prevalence figures, autism stays invisible to policymakers. Caregivers, mostly mothers, form a hidden workforce whose unpaid labour masks the true scale of the crisis.
On the ground
Private social enterprises like Mom's Belief are emerging to offer personalized programs and train parents in behavioral management. This is promising, but it widens inequity: those who can pay get care, those who cannot are left behind. Private players cannot substitute for systemic public investment.
The rural-urban divide
In Tier 1 cities, a family with resources can access a developmental pediatrician, speech therapist, occupational therapist and special educator, though often at separate locations with no coordination. In Tier 2 cities and rural India, none of this infrastructure exists. Families travel hundreds of kilometers for monthly appointments. Telemedicine is expanding assessment access, but therapy delivered remotely for young children requires parental training most families have never received. The result is a two-tier autism system: one for those near an urban private centre, and one for everyone else.
Autism is not exposing a gap in care. It is exposing how poorly we design systems for lifelong human conditions.
What must change
Stop optimising individual services. Start designing the ecosystem. That means one connected care journey from diagnosis to adulthood, not siloed episodes that drop off at age 18; shared data across providers, schools and payers so families stop re-proving disability status at every step; human navigators alongside digital tools, not portals that replace human guidance; real investment in adult autism services, not just early childhood intervention; public-private partnerships paired with government accountability for inclusive education; autistic individuals on policy boards (participatory design, not top-down mandates); and recognition of caregivers as partners who need support, not unpaid substitutes for professionals.
If we can fix autism care, we can fix a large part of the healthcare system itself. Right now, we are not even close.
India's autism crisis is not just a funding gap. It is a design failure. A system built for episodic care cannot handle lifelong conditions: it's fragmented, poorly coordinated, and sustained by invisible caregiver labour. Adding more resources to this system will not fix it. It needs to be redesigned from the ground up.