India's biggest healthcare bet isn't a hospital
While the headlines obsess over new AIIMS launches and IPO-ready hospital chains, India is quietly running a much bigger play: rebuilding healthcare from the bottom up.
The real action is happening in 1.85 lakh wellness centers, on the phones of 7 lakh ASHAs, and inside a vaccine register almost no one outside the ministry talks about. If your strategy still treats Indian healthcare as a hospital game, you're betting on the apex while the base is being rebuilt under your feet.
The architecture
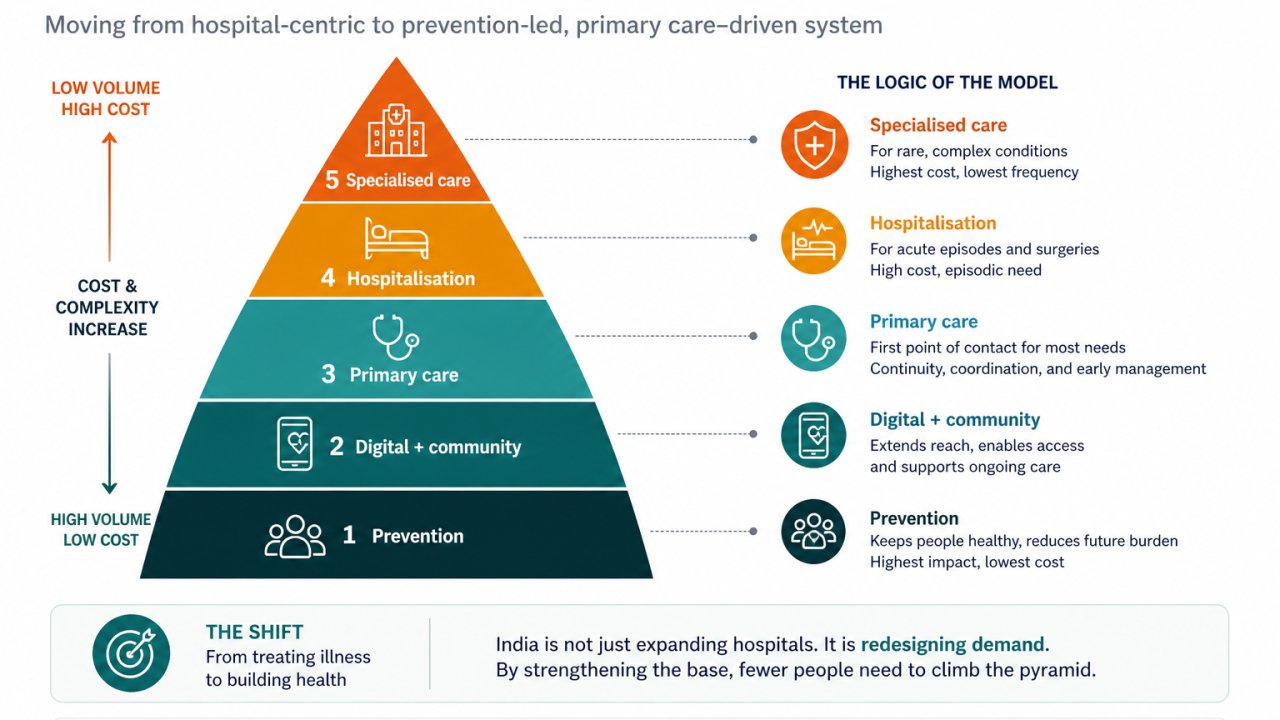
India's healthcare system reads cleanly as a five-level pyramid: prevention at scale (public health, screening, immunization); digital and community (ABDM, ABHA, eSanjeevani, ASHAs/ANMs/CHOs); the primary care backbone (1.85 lakh Ayushman Arogya Mandirs); hospitalisation and protection (PM-JAY's ₹5L cover for the bottom 40%); and specialized care (AIIMS, PMSSY, super-specialty and critical care).
The interesting move isn't at the top. It's at the bottom, where India is engineering the system to absorb 80–90% of demand before it ever reaches a hospital ward. That's a structural break from how health systems are usually expanded, and it's straight out of the WHO playbook on universal health coverage.
Eight numbers that tell the real story
of all deaths in India now driven by non-communicable diseases. Prevention is no longer optional.
Ayushman Arogya Mandirs functional, with 494.71 crore cumulative footfalls.
ABHAs created on India's national digital health backbone.
in PM-JAY admission value authorized, across 11.69 crore admissions.
out-of-pocket expenditure share, down from 62.6% in FY15.
of PM-JAY value already flows to private hospitals.
eSanjeevani teleconsultations delivered.
ASHAs trained for population-scale chronic disease screening.
These aren't supporting metrics. They are the system.
Three things most people get wrong
It isn't. Roughly 56% of authorized PM-JAY admission value flows to private hospitals. In practice it's a publicly-financed bridge into the private hospital network, and that's the most consequential thing about it. Stop treating it as a government program. Treat it as financing infrastructure.
ID creation flatters the dashboard. The harder metric nobody is publishing is consented record exchange per active patient, plus actual workflow adoption inside facilities. ABDM has built the rails. The next phase is judged on whether the trains run. If you're tracking ID counts, you're tracking the wrong thing.
Workforce is. PRS data notes primary tiers are already serving more population than IPHS norms recommend. Most binding constraints aren't capex, they're skilled people, distributed unevenly across states. Health is a state subject, and so is the gap. The real differentiator over the next five years won't be who builds capacity, but who can staff it, train it, and hold it together at the district level.
So what
Government & policy: Move from inputs to outcomes. Stop publishing facility counts; publish avoidable hospitalizations, consented record exchange, and IPHS-norm staffing gaps.
Private providers: Earn the upper half of the pyramid. The structural opportunity is hospitalisation and specialised care, where half of PM-JAY value already flows. The decade rewards operators, not asset-light networks.
Insurers & payers: Design around the OOPE residual. 39.4% is still high vs peers. The product gap is everything PM-JAY doesn't cover: outpatient, diagnostics, mental health, elder care.
Healthtech & digital: Win on adoption, not on IDs. Build for ASHA/CHO workflows, consent UX and clinic-grade interoperability, the metrics ABDM v2 will actually be judged on.
India isn't just building more hospitals. It's redesigning demand: most needs prevented, detected early, managed locally, financed fairly, and escalated only when genuinely complex.
The boring story is "India is building hospitals." The interesting story is that India is trying to make sure most people never need one.